Since many of you are intimidated by ordinary images with magnification, on top of the post is a 3D model - the result of photogrammetry obtained by an intraoral scanner:
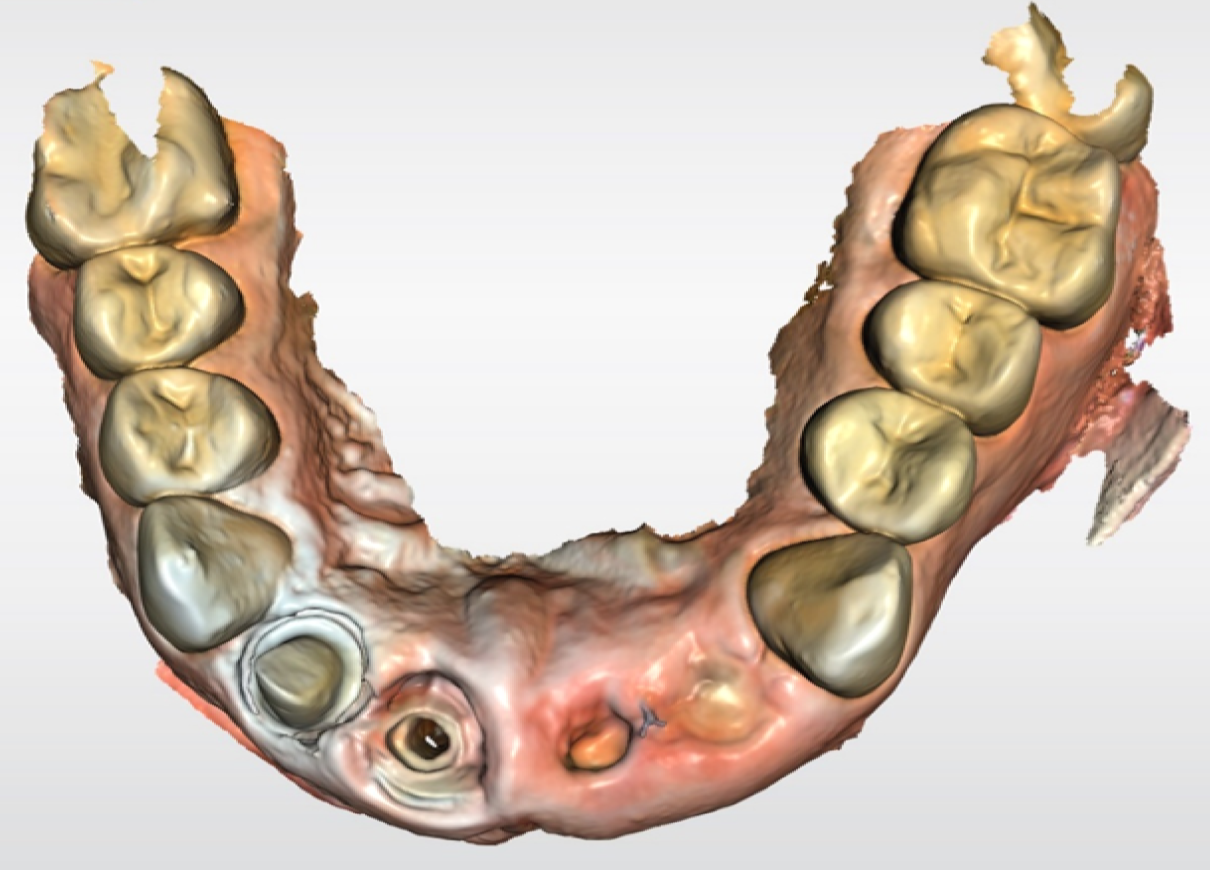
Below there will be photos, so be careful.
From the doorway, the patient said that he had three important business meetings tomorrow and the day after tomorrow, and he would like to smile at them with confidence.
Using this case as an example, I want to show how the conventional level of an ordinary dental clinic, without all the technological toys, differs from what the cutting edge of applied science can provide. We have to make a temporary construction in an hour and a half so that the patient comes out from the first appointment with his teeth. Then there will be an operation to augment the bone using the bull's material (devoid of this bull's antigens), transplantation of a gum fragment, creating a second highly aesthetic temporary construction while the implant takes root.
To begin with, let's pay attention to the condition in which the patient was admitted.

This condition is on the third day after the injury. The patient received first aid within a few hours after being hit with a blunt object in the upper jaw area. The black and blue "cross" is the suture material, that is, the threads with which the wound was sewn up. The photo shows that the surgeon did a good job and, most importantly, did not touch the patient's tooth roots.
The part of the tooth that you usually refer to as the actual tooth is the crown. It is located above the gum. About two-thirds of the tooth is the root, and it is important to preserve it, because it is the root that distributes the load correctly. If the roots of the teeth are preserved, then implants can be placed directly into their holes immediately after removal, simply by creating a new crown to replace the lost biological one. If not, a much more complex operation will be required.

After examining the oral cavity, we performed X-ray diagnostics using targeted images and CT (made a 3D image). There was a suspicion of a crack in one more tooth, and, alas, it was confirmed.
Root fissure is a direct indication for tooth extraction. It means the depressurization of the tooth (in our case, much below the level of the gums). Immediately, perhaps, nothing hurts, but later in this area the inflammatory process will inevitably begin. It is impossible to seal the tooth back: access with such cracks is possible only through the bone, that is, the operation itself will create more problems than a crack. At the current moment in the development of science and technology, the tooth is being removed. Which is what we did.

Here you can clearly see the crack on the cutter, which is closest to the center of the frame. The roughly horizontal line is part of it.
A pin-and-stump inlay made of gold is visible on the adjacent tooth. This is one of the ways to restore a badly damaged tooth. That is, the patient had previously installed a tab on the post. The material was chosen as biologically inert, that is, it does not create additional difficulties with rejection or migration into adjacent tissues and restoration materials. This is a good reliable technology of the past generation, and here the tab was installed very well. Such tabs are placed in many places in Russia, including leading clinics in Moscow. But in our clinics, we rarely resort to this method of treatment, since there are already composite materials and fiberglass pins. The fact is that the golden structure is rather difficult to cover: under certain lighting conditions it is visible inside the tooth, which does not create the most beautiful effect.It is difficult to notice in an ordinary short conversation with a stranger, but the difference in color is a little annoying. Doctors, however, immediately confidently diagnose her from the first seconds of the conversation. Nevertheless, this gold inlay has slightly wider indications, so it remains the last choice for compromise restoration of a tooth: this is when it already needs to be pulled out, but the patient is ready to put up with an aesthetic problem so as not to remove it.
This tab is important to us, because the patient wants to leave the clinic with teeth and go to a business meeting. She will be the support for the temporary structure.

Then I take a 3D model of the patient's mouth and design new teeth for him. The simulation takes about 15 minutes, a lot is automated there. The temporary construction for long-term wear (four to six months maximum) is made from a polymer parallelepiped in a CNC machine with a 4-axis cutter. This thing is called "Cerek" and can be found in different dental clinics. If we are talking about regional, then more often it is a VIP clinic. One temporary tooth costs from nine thousand rubles (more if the design is complex or the material is trickier). Our patient received three teeth just to walk with them for three days. He already knew that after three days he would need a highly aesthetic long-term design to walk with it for five to six months before placing the crowns on the implants.

A conventional clinic can make such a temporary design in the laboratory. As a rule, an impression of the teeth is taken (that is, the panoramic photo is replaced by the introduction of the mass and the removal of the impression), and manual grinding of the teeth is already performed on it. I also use a manual cutter, but only for additional correction: sometimes you need to slightly correct the resulting structure. Since clinics usually rarely keep CNC machines in their premises, this is not done on the day of the visit.
My patient received teeth in about 50 minutes after projection. In total, he spent about an hour and a half in the office: this including examination, hardware diagnostics, removal of the restoration, design of a temporary structure, milling, additional correction and installation, and then - instructions before the upcoming operation.

He came out like this. The design looks good enough, but this is not the limit of aesthetics available in the luxury class: you can improve the color gradient and make the tab invisible in certain lighting conditions. But for the patient's tasks at the moment this is enough.
Three days later, a technologically complex operation lay ahead.
Operation: simultaneous installation of implants
Since the patient had recently lost his teeth, the bone tissue at the site of the injury did not have time to shrink. This is important because bone resorption prevents implants from being placed immediately. Usually, you first need to build up the bone (augmentation takes at least two to three months), and then implants (put screws on which the crowns will hold), which will also take root for a while. And only after about a year, the patient receives new teeth.
Due to the very fast patient's treatment, we were able to perform a one-step installation of the implants, that is, immediately "screw in the screws", which will be the attachment points for the "new teeth". Implants are tubes with two applied threads: one external for attaching to the bone and one internal for installing the structure there later. That is, we create slots in the bone, where we can install whatever we want later.
The diameter of the implant is less than the diameter of the socket that remains from the tooth. Conventionally, if you do not fill the hole with something, then tissue collapse will occur. Therefore, we immediately add new bone around the implant so that it, so to speak, matches the physiology of a normal tooth (as far as possible), that is, the new "thin" tooth is surrounded by bone. To do this, we put a graft there - a bone-substituting material made from the bone of a bull, from which all donor proteins were chemically removed. The graft is a granule that is actually used by the body as a scaffold to create a new natural bone at this location.
It happens like this: as a result of the osteoblastic jump, it turns out that the vessels begin to grow from the gum to the implant through the graft. This type of vascularization is only possible with fresh injuries. If the teeth are removed without the immediate installation of implants, then you need to wait for stabilization - at least primary mineralization. This is eight weeks, and only then can the implant be placed.
If the patient had their teeth removed on the spot and he came to us with the extracted teeth, then the tissue loss would be very high after stabilization. After tooth extraction, one month later, tissues from the vestibular side collapse by about 30–40%. At the same time, on the palatal side, it is insignificant: there is good nutrition. It is not a fact that a deficiency of bone tissue would be critical, but in any case it means an increase in risks, which neither we nor the patient need. Immediate implantation, if possible, is the best medical choice.
Preparation for surgery begins with the design of implants in a virtual environment:


Don't be alarmed, these are their axes.
We used this time to good use: based on the complete diagnostic data, we already had accurate models of the oral cavity, bones and blood vessels, thanks to which we were able to position the implants optimally. We have chosen two attachment points and prepared all the necessary calculations. Then we created a navigation template - a piece that is installed in the mouth during the operation and does not allow you to make a mistake even by half a degree. Usually the template looks like this (this is a different template, for six implants, I did not photograph the template of this patient):

More precisely, we photographed it already during the operation, this is how it is applied:

It is done on this printer:

Design software - 3Diagnosys and PlastyCAD. Not every clinic can afford a printer in dentistry either. The fact is that as soon as the inscription "medical" appears on any device, its cost goes to heaven. The printer costs about three to four times the price of a similar industrial printer of the same accuracy and the same grade, but is certified for use in the clinic. And it looks a little more impressive.
Conventional dentistry orders a navigation template from a laboratory somewhere in the city and usually receives it after seven days. We produce templates on site very quickly: sometimes we need to. If you are interested in more about navigational surgery, then my colleague has just developed several new approaches, here is a post about his scientific work.
Next, we plan the operation: what may be required, what are the possible risks, what to do when such a risk is realized (and how to remove it) - in general, we are preparing a strategic offensive plan with all the options. I heard that sometimes critical medical software is updated in about the same way: “What if the light is turned off?”, “What if it doesn’t get up until 5:30 in the morning?” - etc.
Our printer is the fastest on the market, taking about 20 minutes to complete a template.
We are also preparing a highly aesthetic long-term temporary construction. This is about the same as what we did at Cerek, and from the point of view of common medical sense, it is already redundant. But the patient insisted that during those few months that the implants would take root, he would like to have beautiful front teeth.

Here it is necessary to explain how the temporary construction differs from the permanent one and how the highly aesthetic one differs from the usual Cerekovsky one. If a patient turned to a regular regional clinic with a lower technological level or chose cheaper options, then he would be offered a bridge structure with attachment to the remaining teeth as one of the options. To simplify greatly, both of our temporary constructions are approximately similar in principle to such an analogue, only they are made of polymers, which after two or three years of wearing will begin to be destroyed by bacteria. They can be worn for a maximum of six months. They should not be used as permanent ones, not only for this reason: fulcrum and load distribution are also important. If we want the patient to continue to be able to chew for the rest of his life (usually more than two or three years), then we still need to set everything up like this,so that the load falls on the tooth (or the bone under it) as evenly as possible. Therefore, implants are needed.
The highly aesthetic design differs from the usual for the patient primarily in color. The teeth have a dark color in the lower part of the crown, then they brighten, and at the edge they become almost transparent. It may seem that this is not very noticeable, but the teeth of the temporary construction are made of polymer of the same color, which makes them stand out in photographs and in one-on-one conversations. We had a case when a wife did not want her husband to know that she was changing her teeth for implants, and it was with a highly aesthetic design that she confidently hid it.
The material of the Cerekov construction is PMMA, it is also polymethyl methacrylate, it is also plexiglass. Now Cerek has learned how to make it with a color gradient: blocks come in different colors and different transparency. This allows them to compete with highly aesthetic designs of the correct colors, but in January 2021 such blocks have not yet arrived in Russia in principle.
Next, my colleague, surgeon Andrei, takes over the patient:



I removed unnecessary residues, applied a template (photo above), placed implants:

Now pay attention to what is near them:

Graft granules are visible near two metal screws (the same prefabricated bone at a temperature of 450 degrees). If there were three attachment points, then there would be no place for the germination of soft tissues, the intergingival papillae would not form, and there would be no natural aesthetics. I took some bone graft and a gum graft from the tubercle behind the seventh tooth. This was necessary to compensate for tissues in other places that were lost in the trauma. The photo shows how he moved the pieces of gum to the correct places.
Further - the seams:

And the design:

The patient flew to another city the next day.
Why was the patient able to fly away immediately after the operation?
In general, this is not the best idea, but there were no contraindications to this. Everything stopped hurting the patient even after the first aid. During the operation, he was under local anesthesia (we use articaine drugs) and did not feel anything. After the operation, Andrey prescribed him amoxiclav and a non-steroidal anti-inflammatory + pain reliever (an analogue of ibuprofen).
Amoxiclav is a protected penicillin, one of the safest broad-spectrum antibiotics in the world, and is prescribed even for pregnant women. Lincomycin is also loved in dentistry.
The patient will be able to feel something only on the fourth day (when nothing will hurt), because before that he takes NSAIDs. If secondary inflammation suddenly began as a result of bacteriological damage (usually this does not happen, but this is a well-known postoperative complication), then it will begin much later, when amoxiclav is excreted from the body. Examination of the patient - in two weeks, then the stitches are removed.
PTFE suture is a gortex-type membrane material, very clean, tough, elastic, soft, hygienic. It is pulled out in one motion, all together they removed 30 seconds from under the temporary crowns.
The next checkpoint is complete healing, which is four months after the intervention. If we see that the bone is of high quality, there is nourishment from the vessels from the palate and cheek, the vessels have sprouted correctly inside the graft and anchored, osteoclasts have passed through these vessels and built up the natural human bone around, then everything is in order. Usually, abundant vascularization is noticeable in the fourth to sixth week (primary - in the second week). Mineralization begins from the sixth to the eighth week.
The patient is waiting for his crowns (they were calculated when planning the operation), they just need to be screwed in. They will fit very accurately, since immediately after the diagnosis we thought over the entire aesthetics of the future jaw and precisely made the navigation for the surgeon. Implants can be placed manually without a template, but we put them in order for the patient to eat and smile beautifully. Precise positioning in the anterior region is necessary: the bite is different, the exit of the teeth is different, in order to place it clearly so that the shafts do not come out on the anterior surface of the crown - only a template.

Navigation template.
Medical advice: how to avoid such a case
Moral of the story: If possible, avoid meeting trees during active sports.
PS If you get to our clinics, then say that you are from Habr, there will be a 5% discount. And write down the phone number +7 (916) 740-20-08, if there is an injury, we will be able to advise you right while you are standing with your teeth in your hands, sometimes it helps to save 300-400 thousand rubles, depending on your plans.