
Caries at the initial stage, the teeth on which the tissue will be removed are isolated with a rubber dam. This is so obvious, simple, and so improves the result of even simple interventions that in the regions you will be burned at the stake for the mere thought of doing this constantly.
It started with the fact that we brought operating microscopes. Today, doctors in my clinic do not work without them in principle. And this is causing a pretty strong holivar even among the very experienced dentists on the market. The first practical result was that we greatly reduced the percentage of complications, and the patients quickly (in about a year) understood this from the reviews. We started earning a lot more.
Or here are devices for flowmetry and ultraviolet radiation of tissues. Why, when there is an X-ray or CT scan? And then, that there are pregnant women who are treated for caries when the problem is pulpitis. That is, they simply cannot correctly diagnose the problem without a snapshot, but we can.
We have 3D printers. We print navigation templates with holes on them to insert into your mouth the shape obtained by photogrammetry (panoramic shooting with a camera inside the mouth). They stand up almost with a click exactly on the teeth and give accuracy up to hundredths of a millimeter in the positioning of implants. We still have many toys, but the main change in medicine and dentistry is not in them.
The main thing is that the scientific approach has changed approximately with the advent of the Internet. And we in Russia are 30 years behind in our conservatism. But I did not come here to whine, so I will tell and show with specific examples the problems of punitive dentistry and possible solutions. If you're willing to invest in applied science, of course.
Simple navigation template: printed on the patient's side on a 3D printer and ensures that the drill goes at the right angle, does not slip and goes to the right depth.
What are we doing
I now have one of the most technologically advanced dental clinics in Russia (and we are in the top two percent in the world). This was not the case once. We were once young and wanted to improve the world. And we are very fortunate that we were familiar with the abhorrent capitalist models, where businessmen do something good just for the money. It quickly became clear that it was possible to earn money on applied science. Especially when you have a staff of doctors who can do something that is not done anywhere else on the continent. More precisely, you do not earn on this, but on the flow of patients who appreciate that people with hands from the right place work with them.
The Soviet framework assumes that civil medicine is a creative profession. The Western framework tells us that any medical situation consists of three parts: diagnosis, case selection and intervention implementation.
Diagnostics is when you understand correctly what exactly is wrong with the patient. Case selection is when you have chosen the best method of intervention for this patient's condition based on your capabilities (devices, materials and skills). Implementation is when you did it right.
Implementation in the USSR has always been excellent. Our doctors have always stood out for their excellent manual skills thanks to their strong school. The diagnosis was normal - not space, but patients rarely died because they were being treated for the wrong thing. But there was always trouble with the choice of a case, because doctors rarely knew how to calculate statistics.
The point is that there is no creativity in medicine. There is the most accurate definition of the situation, identification of significant factors and comparison with significant factors of intervention options. The task is to understand which option and how exactly implemented will be optimal for the patient. To do this, you need to do not what you are best at, and not what you are accustomed to as a doctor, but what has been statistically proven to be effective.
As you know from the situation around vaccines, even seemingly enlightened people can turn out to be still obscurantists in applied aspects.
Moreover, modern science requires the joint action of many doctors in many clinics to generate the same statistics and correct clinical research. And if Europe has all the tools for this, then in Russia I have very little idea of a regional clinic that helps another regional clinic for the glory of someone else's doctor. We simply do not have a medical community ready to jointly develop science. More precisely, in recent years it has appeared, but it is too slow. And its development is greatly slowed down by education, the regulatory framework, and traditions in general.
And also the fact that earning money in science for some time was a shame. And I am of the opinion that medicine can only develop with funding. And in order for someone to finance it, it is necessary that there is a long-term commercial interest in this.
When we became a clinic capable of scaring a middle manager with an account, but with the best equipment in Moscow, it became clear that smart is a new sexy.
What's wrong with the OMS?
That there will be a tooth pulled out.
The main task of the compulsory medical insurance is to reduce mortality at the lowest cost. That is, when there is a choice, to save something with a very complicated procedure or to saw off, usually a part of the body falls into the basin. But if the legs are still somehow trying to save, because it is very bad without legs, then with the teeth the protocol is simple. If it requires more than 15 minutes of intervention, pliers are more practical. I, of course, greatly exaggerate and oversimplify, but with the norm of 15 minutes for a filling in the budget of 220 rubles, you can yourself assess the variability and depth of the doctor's approaches.
OMS usually adapts something very reliable from commercial medicine that is already on stream. Commercial medicine (like public medicine) develops when it is financed. And now all Russian and CIS dentistry is based on enthusiasts. These are people who understand what year they live, take the latest techniques and technologies and integrate them into practice. But there are also those who studied at the institute in the 80s, received a diploma and continue to tear their teeth furiously.
An example about microscopes
These are such devices that completely change the fit of a doctor in dentistry:


Historically, ophthalmologist surgeons started working with them first, because it is rather difficult to go and buy a pair of spare eyes. A person has a lot of teeth, so they came to dentistry later. And if in the case of the eye their use is quite obvious, then in the case of the teeth it still raises questions.
I answer the main ones:
- Yes, they have a different fit and a different angle of work, which means new habits in manual skills. This position relaxes your hands and allows you to work without errors for much longer. Less tremors, less stress at difficult angles, and generally wider access.
- , , . , . , , , . .
- , . 35–40 , . , . .
- , .
- , . , . , . 15 . , , , . , . , ( ) . , : , , ( ). : , . , . . , . 0,2 , 1 . .
- - .
- . , , , . .
For the layman, all this is not very important. The important thing is that we are able to save almost any inflammation. The success rate rose to 90% compared to 60–70% of the usual statistics for root canal retreatment. Such a super important thing appears: if the tooth continues to ache after the intervention in the canal, then you know for sure that it is not the canal. This is critical in order not to open it a second time. Because there is confidence that the cleaning was of high quality.
Look, here is a tooth on a handkerchief that isolates it from saliva (the patient is still attached to the other side of the tooth):

And this is how it is seen through the microscope:

See? The channel is clear.
An example about a scarf
This thing is called either a rubber dam or a rubber dam. A latex plate that isolates the tooth from saliva, air currents from within the patient, and so on. This is the very isolation, for the absence of which in the United States you can sue a dentist. If, after the intervention through the dental canal, you realized that there was no such plate and he worked "live", then you can safely sue him for several million rubles with almost one hundred percent chance.
Guess how often it is used in Russia.
And this despite the fact that there is direct research into how it reduces the side effects of different interventions. And it would be fine if he just reduced them, we love to take risks and are ready to endure pain for saving 10-15 thousand rubles, right? It can be added that this intervention is of a fundamentally different quality: for example, veneers do not fall off with it, the quality of adhesive fixation is an order of magnitude higher.
But if I still see rubber dams in dentistry, then there are almost no navigation templates.
An example about navigation templates
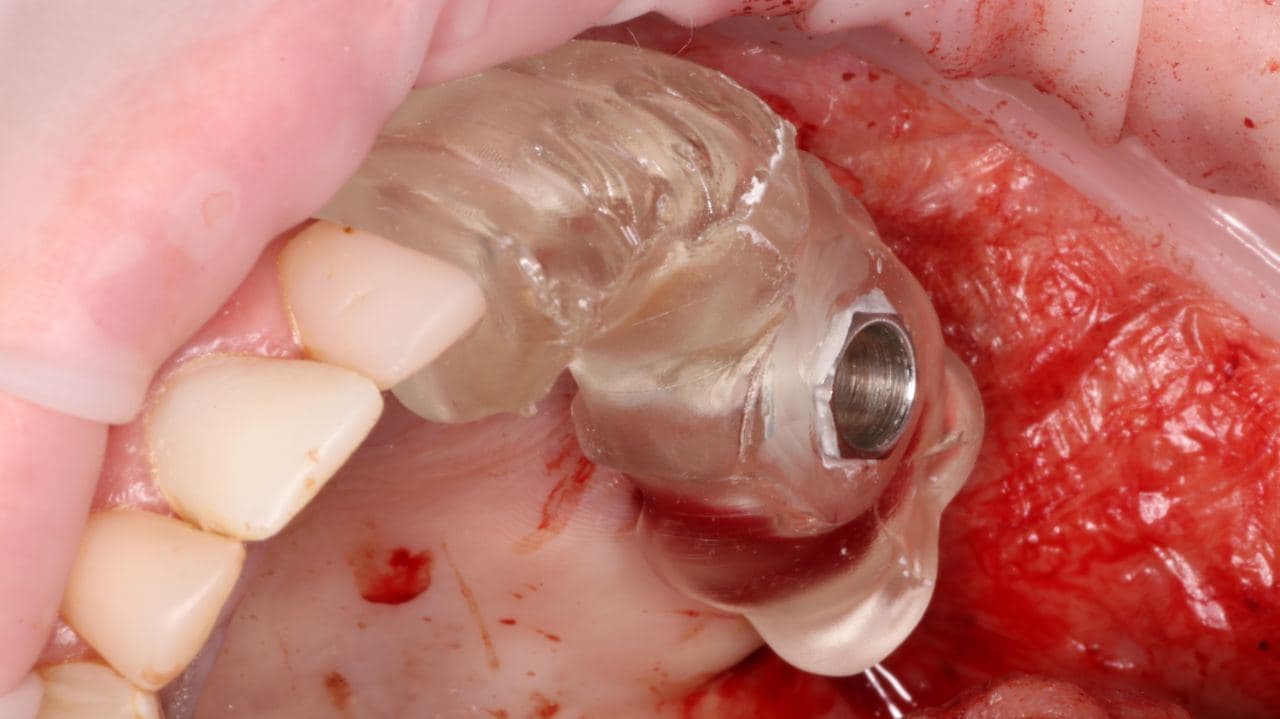
At the top of the post there is one picture, here is another one:
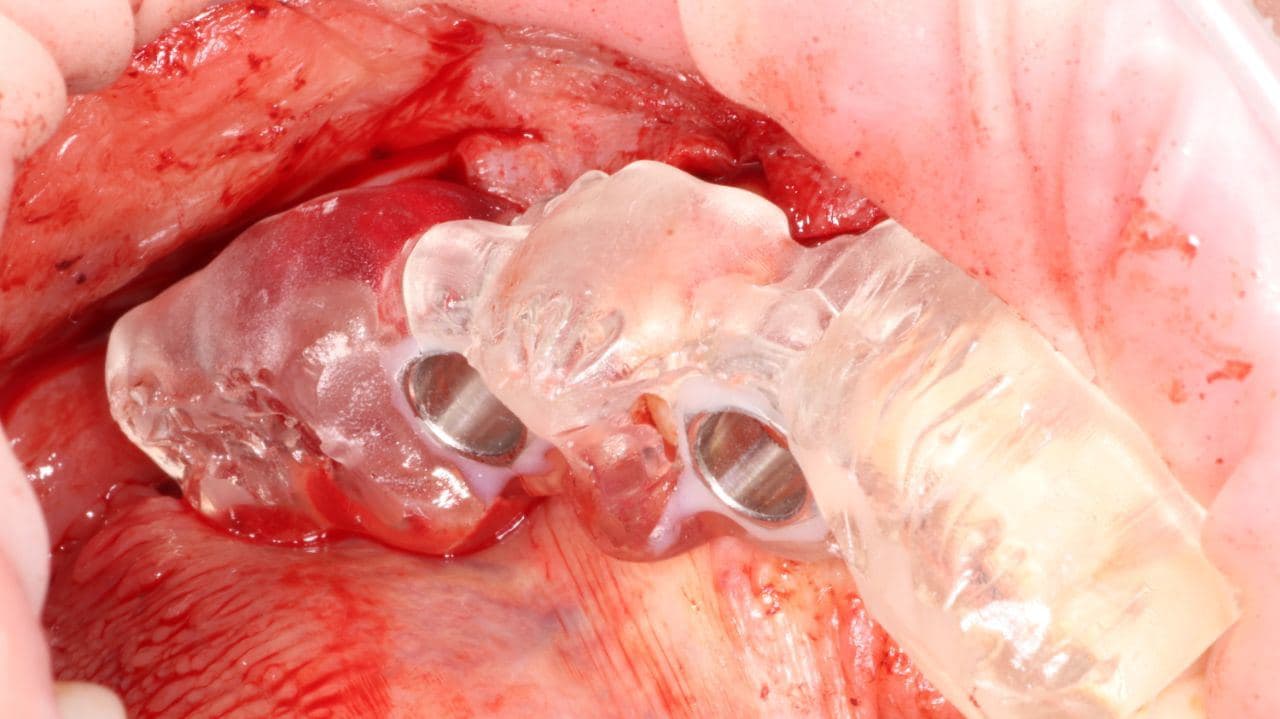
In the photo there is a rather crude template, and my colleague Huseyn nearby wrote about his scientific development of more complex ones. Post here . Briefly: Imagine that you need to place a microimplant in a person. And it would be nice to take such a thin drill, make a hole in the skull from the side of the oral cavity (in the palate, for example) and hit it the first time. And if the patient jerks or something else goes wrong, do not distort anything.
Well, or imagine that you just want to control the drill stroke for easier work.
What does a normal doctor do? He tries to reduce hand tremors with exercises, puts the patient to sleep with anesthesia and takes a thicker drill to get it right. All three methods are commonly used. What are we doing? We charge you dearly for the fact that our medicine is minimally invasive. And we make this very template on a 3D printer, with which you can twitch as much as you want. But usually work on it takes literally seconds, because vzhzhzhzh - and it's done without any second-fifth-sixth approaches.
To make such a template, you need to have normal diagnostics, design software and know mathematics (we developed part of this software for this, you don't need to know mathematics to use it). This is how it looks when planning:
And the installation of the implant according to the template:
It used to be that one doctor places an implant, and the second screws a crown there, and it does not stand at the right angle. With a template, this is basically unrealistic.
Diagnostics
High-resolution CT is understandable.
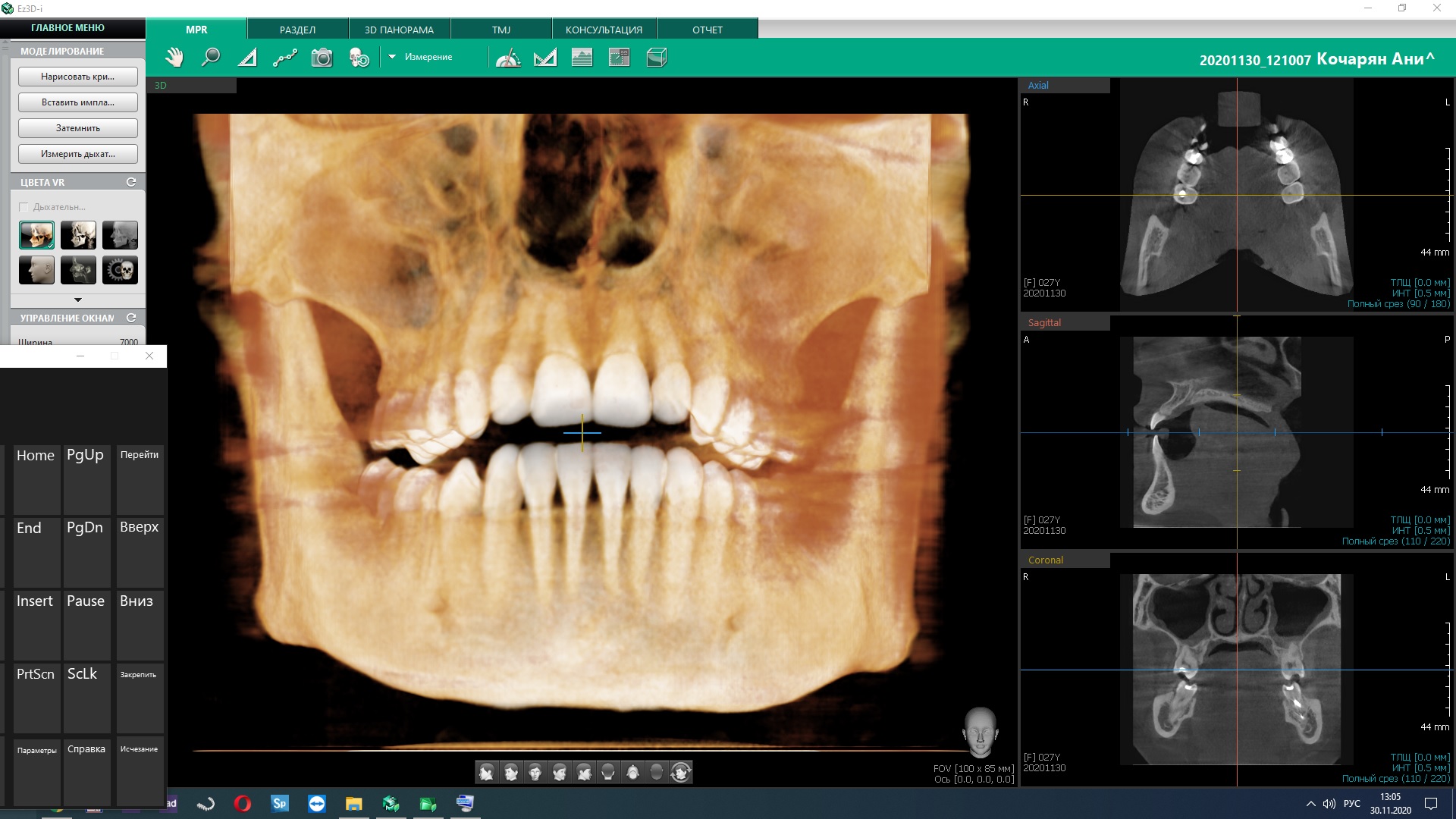
It's important to do it quickly. So I get access to it right in the office while the patient is lying down:

By the way, we do not have paper pictures, but we have negatoscopes (viewing tables). Because these are the requirements of the standards.
You also need a scanning camera, which is inserted into the oral cavity and shoots everything there. Photogrammetry (or 3D scanning through photos) of real teeth is many times better than the same scanning of their impressions.
Including for small children, who often do not give an impression at all. And the camera, even if pushed away, is not scary, we will scan it again, it is very fast.
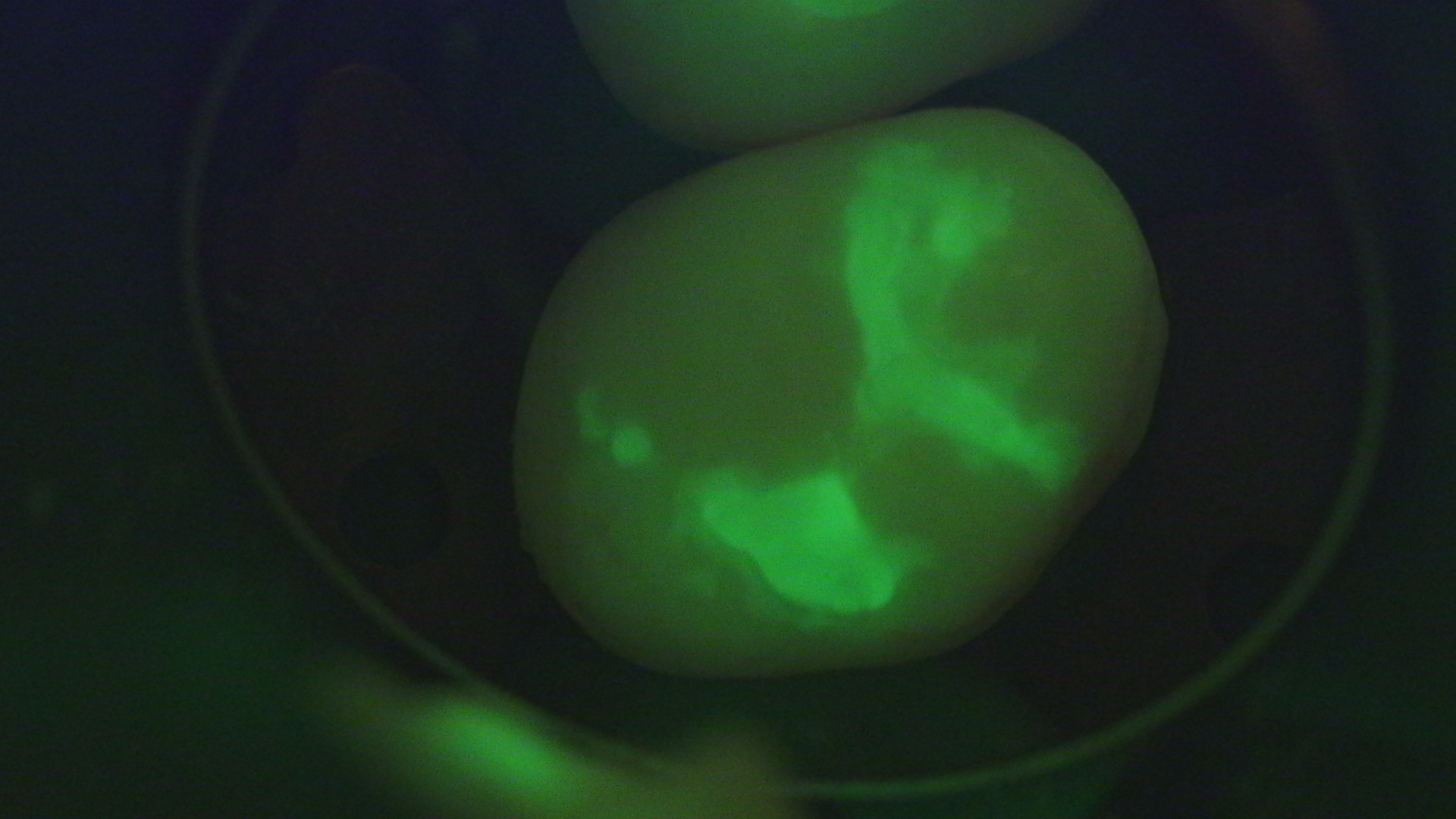
The microscope makes it possible to look at the tooth in different ranges, including in ultraviolet light. Restoration materials are visible here. And here is an example of an ordinary picture for you:
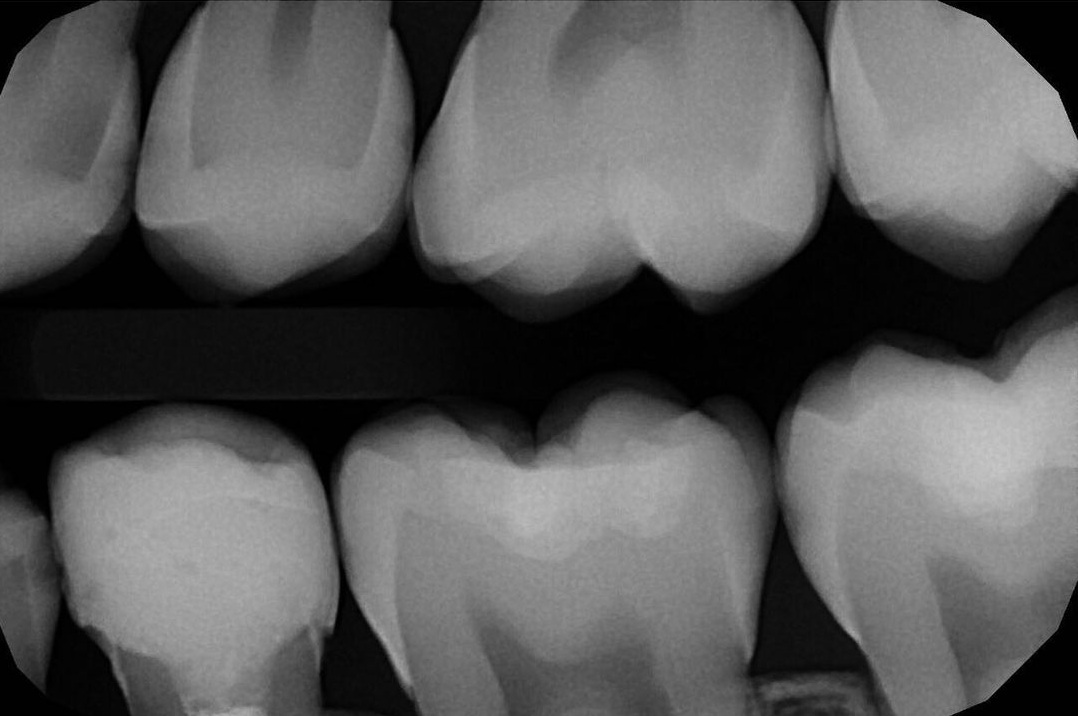
And a similar search for caries with a coloring highlight:

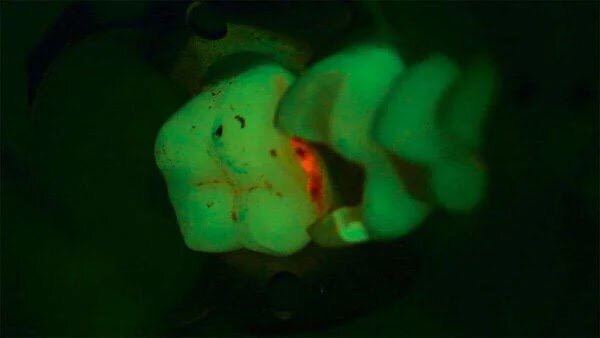
It is useful to have this right in the operating microscope so as not to remove excess tissue. This is not a super breakthrough, but very convenient.
According to US statistics, 80% of caries could have been diagnosed earlier. Therefore, we have, for example, like this:
- Targeted intraoral images.
- Targeted interproximal images.
- CT scan.
- Instrumental examination methods.
If you are frightened by the images in terms of radiation exposure, then I’ll say right away that the amount of images is about 80–150 times less than one pass of that panoramic scanner where you shoved your head in the dentist's office in any average clinic. Because technology.
Interproximal images, where eight contact surfaces are placed on one image at once, are rarely done, and they are important, because the caries is the smallest one. CT scan helps to see all the teeth in volume, in turn, all inflammation is visible. A teleroentgenogram is done mainly by orthodontists or with complex orthopedic treatment. This is a special study for anthropometric research, that is, it gives a one-to-one head image, and angular measurements of the magnitude can be made. The photo protocol is important for before and after comparisons because it is important for both patient and clinician to learn. If there is no photo protocol, then after a few years it will be difficult to restore the picture.
So, what is wrong with domestic medicine?
The problem is not that there is no technology. They are there, these devices, we brought them in and installed them, no one bothers to repeat them. The problem is that a different mindset has to come along with the devices.
I like countries where they invest in research and development, where doctors begin to lecture based on their experience, summarizing it numerically and conclusively. Where all dentistry is based strictly on scientific evidence.
We have it in many ways homegrown. Historically, "as dad did, so I will do." And in scientific medicine, a physician's personal experience is the least reliable source. It is necessary to do not as dad advised, but to come up with a method, test it with the patient's consent, ask 100 doctors to apply the same method in the same situation, collect data, independently measure and evaluate the result, describe it, prove it and try to refute it. Then over time it becomes a system. And the system turns into a routine. There is no creativity in the routine - there is a predictable result.
Our system stops at about the point when it is necessary to move away from the patterns of institute education and learn something new that has happened in the world. To do this, you need to take courses from a doctor who has worked out and scientifically substantiated the method. Perhaps I am cruel, but the compulsory medical insurance will not allow doctors even to earn money for regular advanced training courses.
How to collect 100 cases in Russia for statistics and substantiation of the method? Or to work for 15 years, and then it will become outdated. Or falsify, which in practice happens much more often. I like the system when the doctor works out about 40 cases and then tells the community: look, it seems to be working. Try it yourself. This is in the American school, in the German one. Arranged a little differently, but the important thing is that there is evidence. Each time you expand your knowledge: if the doctor did not know the other two methods, then a typical one from the institute would come up. And here the doctor thinks and understands why and why he does this or that manipulation. This is “case selection” - an ability that is often not available in regional medicine.
This is important because there is the same soft-touch method in augmentation. He has a known complication rate (very small), almost no risks, a good success rate. That is, having done everything according to the technology, you will know for sure that if it didn’t work out, your hands are crooked, and not with the method that something is wrong. This provides quick feedback. I know many doctors who work with methods with seventy percent statistical success, but they do not count statistics for periods, because it is scary. But it is important to know where you missed, and if so, the same video recording from the microscope will help to analyze the case with colleagues.
The next feature is underdiagnosis combined with a low culture of communication. The doctor rarely explains what he does, why he does it, and how he does it. The doctor rarely conducts diagnostics in search of the cause of the disease. It's like coming to an otolaryngologist with a runny nose, and he will cure it only in the right nostril, because there were no complaints on the left. In principle, it should not be such that a patient leaves without knowing his diagnoses. In our country, more often than not the doctor tells the patient what to treat, but the patient answers the question: "Well, what are we doing today?"
In aesthetic dentistry, normal plans and explanations are needed, why all this is and what it will lead to:

Here in the pictures - the states "It was", the calculated projection, the render of expectations and at the end of the photo "It has become".
Do you know why such plans are often not fixed? Because it requires working out good interdisciplinary interaction. We have almost no collegial decisions, it is the doctor to whom the patient turns to decide whether or not to keep the teeth. Therefore, do not start with a surgeon in small clinics; by the way, his choice of case is pretty straightforward.
But there is progress. I see how enthusiasts unite and move science. I see how the market shoves people: its requirements change. Thirty years ago, people wanted it to be free of a crack, the mouth did not look like a battlefield, and the treatment was at least not very painful. Then the lurch into comfort went, and finally now grandfathers come who want to chew a steak. And they know that it is possible. And people who like looking good. Understanding that there will be no pain. By the way, yes, we can do everything in a dream or under nitrous oxide, when you laugh like a Viking rejoicing in battle (the main thing here is not to overdo it). By the way, yes, shallow anesthesia and medication sleep: we can put you to sleep and treat you under local anesthesia. We are able to erase your memory of manipulations (we are talking about sedation with propofol). This is despite the factthat even a biopsy is taken in the OMS without propofol, because the patient's pain does not affect his survival. He will be patient. In practice, this means that children are not afraid of the doctor, because they love to be "fighter pilots" or watch cartoons under nitrous oxide. And adults are ready for complex manipulations with the understanding that they will not have to suffer.
In general, there is now a big shift towards improving the quality of life about “not having to suffer”. In our country, for example, almost any oncology is still a sentence, a fate. In the USA and Germany, the attitude is this: it is just a disease, it must be cured in time and the quality of life must be maintained. It happens, but it's not as scary as it could be. This had a very big impact on the temporary restoration, when the patient's teeth are taken out and they are not released in this form, but something is put to chew on leaving the clinic. And then the temporary is changed to a permanent one, but the patient never leaves the clinic without teeth. We had a woman whose husband did not notice how her six teeth were changed.
We do what we can and talk about it. This also changes the situation.
Everything is beautiful, but what does a really dangerous research look like?
In dentistry we have such a thing as BMP-1, aka Bone morphogenetic protein. It looked like a promising technology for tissue augmentation with the cells of the patient himself. But somehow people started dying after the dentist's appointment. They came up with a second version: they make an incision, put a sponge with BMP-2, and it starts to grow. The problem is that it is not clear how to stop this growth. And it is not clear what is growing: it is not always a bone. They have not yet learned how to fully control the process, but it is necessary to conduct experiments.
The Russian approach is to do illegal operations.
And you can negotiate with homeless people, they often do not mind training a surgeon for money that is converted into vodka. Or negotiate with prisoners, and so on. In Russia, again, there was a history of teaching implantology through foreign trips. They took a group of young surgeons, took them to Sri Lanka, where they gave people teeth for free. The surgeons were just filling their hand. People were happy because new teeth were free. I saw a tour to Brazil in the village: you come, there is an office, people understand that you are a novice doctor, but they trust you more than the local healer.
If all participants in the process understand the risks, it is probably better than when you come to the clinic, and you are not told that the surgeon is doing this method for the first time. Or at least when they load a new doctor with a discount, explaining the discount by the fact that he is new, and not cut, as usual, without explanation.
In general, we have a struggle every day here. If you are interested further about the science in dentistry - stay with us. The next post will be about what exactly we charge good money for and why it is critically important not to give a doctor a premium depending on the amount of gold pins installed. In the meantime, just in case, I note that you can do science in Russia, it's interesting, you can make money on it, but you can improve a lot. And I personally would like that.