Caution / Caution / Achtung: under the cut, not the most aesthetic photographs of eye surgery are carefully hidden in spoilers. If you didn't like playing as Orbb in Quake III Arena (pictured above), then looking into the spoilers is not recommended.
We were faced with an interesting experience that might be useful to some of the readers - initially I understood that I would want to write an article about this (as well as about previous experiments with vision). On all days of visiting the clinic, I walked with my tail to all the offices: I asked questions, reeled information on my mustache, dictated voice messages to myself in a telegram (so as not to forget the details), took pictures of every step. Therefore, everywhere it will be written in the plural - "we went", "we were led", etc.
Training
Before the operation, the beginning was the same as mine: measuring the pressure (120 to 80) and a couple of drops inside for peace of mind. Well, a couple of drops of inocaine in the eye - anesthetic for the next stage.

Then we go to the room where the diagnostics were carried out. Only this time, not for diagnostics, but for "eye marking" - Tatiana Shilova's assistant asks another colleague to " make a marking of zero one hundred and eighty for both eyes ." We are talking about a marking axis passing through 0 and 180 degrees - this marking will serve as a guide when installing the lenses. Because not everyone knows that there is such a thing as "cyclotorsion". That is, the rotation of the eye around its axis when moving from a vertical position to a horizontal one. It is just the markup that allows us to take into account cycling.
The doctor repeatedly drips anesthetic drops, and then, with a special marker through a slit lamp, makes small purple lines-marks in the region of the limbus (the place where the cornea passes into the sclera). If you blink, then they will not wear off, but if you rub with your hands, they can.

Then we were sent to the waiting room. The most painful period - you understand that such changes are about to occur that a couple of drops are simply not able to get rid of worries) Dad is trying to get distracted in the phone - again I pay attention to how he squints, trying to see something on the screen. Fuh, I hope this will soon become a thing of the past ...
By the way, while we were waiting, we added midrimax - special drops that drip during diagnostics and before operations.
Operation
They turned on the “green light” for photographing all the previous stages, but, unfortunately, I was not allowed into the operating room. Not because there are some secrets (especially since I was there for the operation, what secrets)), but because this is an operating room - the room must be sterile and there is no place for outsiders. But there is also good news - Alexey Ivanovich Shilov, the head of the clinic, agreed to take pictures.
So what was happening there.
At the very beginning, the surgical field is treated with a skin antiseptic several times for sterility. The patient is completely covered with a sterile blanket to prevent microbes and viruses from entering the operating field. For the eye, the bedspread has a window with a film and a pocket for collecting liquid. A small incision is made in it and its edges are glued to the eyelashes, since the biggest source of any infections is just eyelashes. The eyelids are moved apart with the help of an eyelid dilator - a special spring, which is known to everyone who has ever gone to the operating table at an ophthalmologist. That's it - you can't accidentally blink or close your eyes.

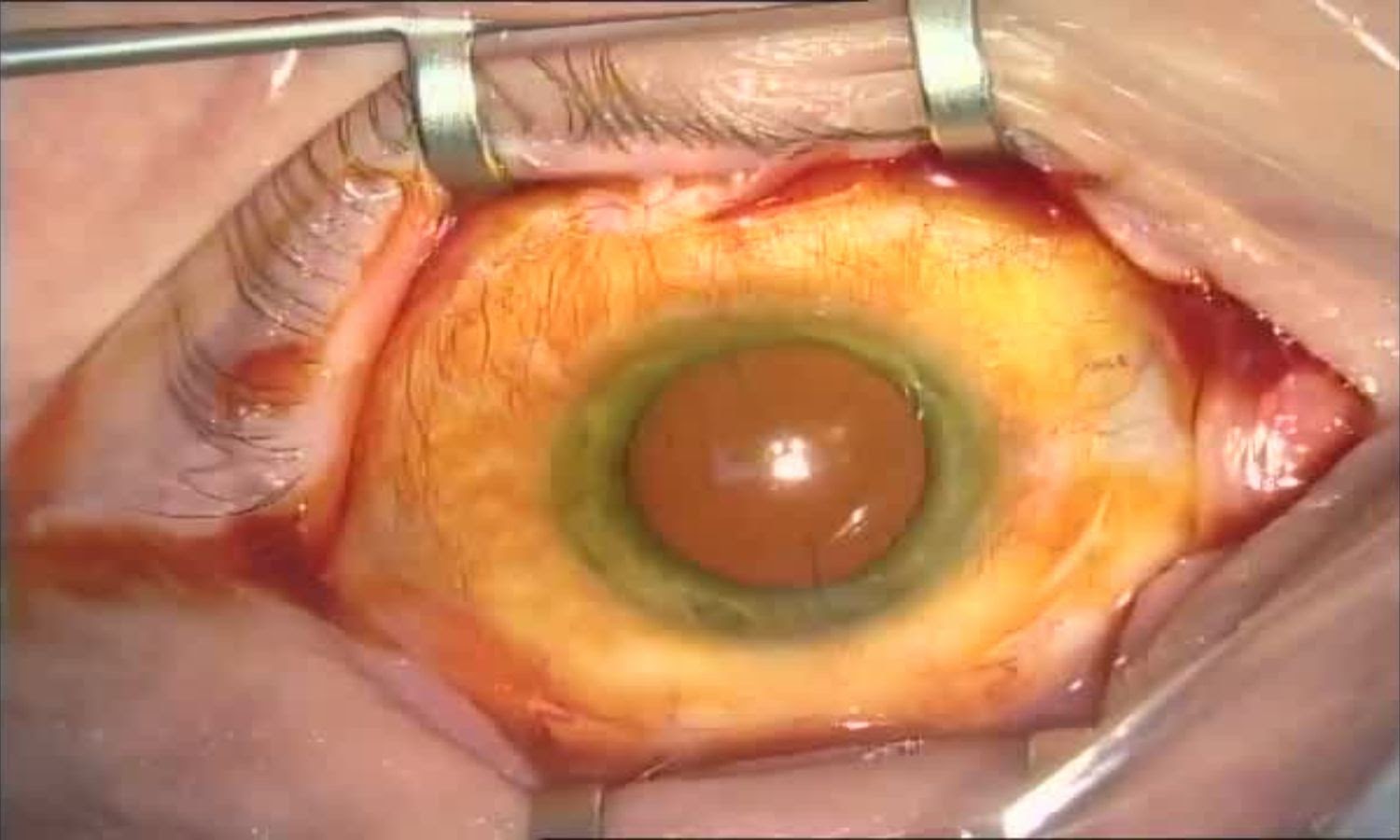
Initial state of the eye

Eye treatment with betadine (antiseptic)
In front of Tatyana Yurievna there is a microscope - a picture from it through an optical divider is displayed in two places at once: directly to the surgeon and to the camera matrix (through which the protocol of the operation is written and optionally displayed on an external screen - just part of the photo was taken from it). By the way, the microscope is also capable of projecting the axes for implantation, but in the eyes after keratotomy Tatyana Yurievna necessarily duplicates the markings - for double control.

The first instrument in the hands of the surgeon during the operation is a diamond ophthalmic knife (aka scalpel or spear). An expensive and damn sharp thing with a diamond cut, or even completely made of a solid synthetic diamond. Today, disposable keratoma knives are a good substitute. They make two small (less than 1 mm) stepped puncture inlets in the cornea, through which manipulations take place, and one main entrance of 1.8 mm - it is needed for the introduction of an ultrasonic needle and through it the IOL will be installed in the future.
Keratom knife (size 20G) in action

The cut diameter is chosen depending on the lens: some are flexible and can be rolled into a thin tube to make an injection through a very small hole; some are less flexible and need a larger cut. Usually surgeons use an entrance of 2.2 - 2.5 - 2.7 mm, but Tatiana Yurievna works through the smallest possible - less than 2 mm. In this case, size matters: the smaller the better.
The main incision is formed

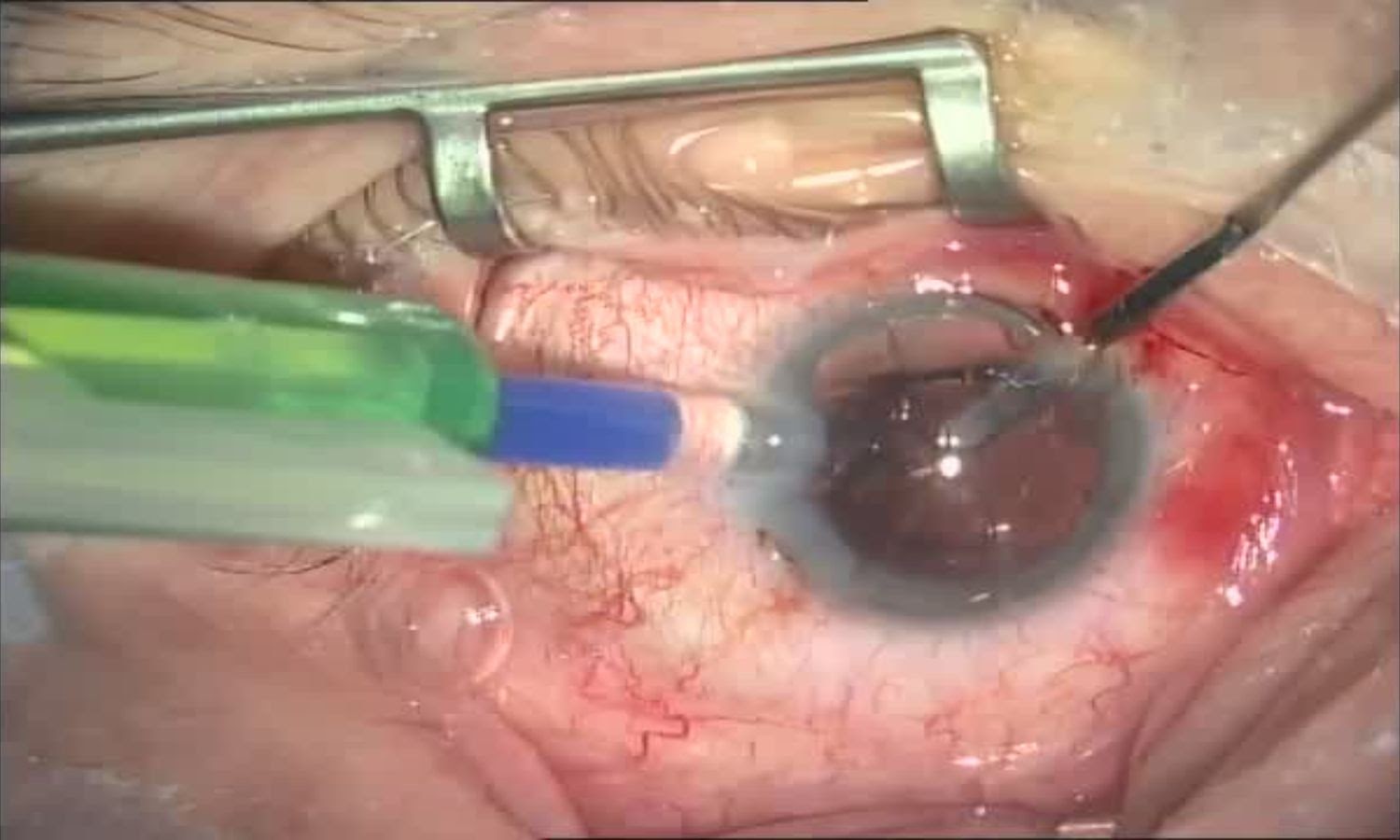
Immediately after opening the eye, solutions are injected into its anterior chamber: anesthetic, pupil dilator and even a special dye for the lens capsule. Staining is needed for those who "suffered" cataracts and they have matured, impairing the reflex from the fundus and thus creating additional problems for themselves and the surgeon. Dad, by the way, did not paint anything, since we came "on time".
Introduction of viscoelastic into the anterior chamber

Then a viscous protector is injected: a special viscous liquid to reduce the risk of damage to surrounding tissues during cataract surgery and to create volume inside the eye. If this is not done, then you can damage the cornea from the inside and then a person, even with a new lens, may remain blind. Viscous liquids have different properties: some spread and envelop tissues, others are tight and dense (these are either special natural extracts of hyaluronic acid of different concentrations - such as "extract" from the scallops, or artificially synthesized, like methylcellulose). By the way, the operation of phacoemulsification itself was developed in the 70s of the last century, but it became safe precisely thanks to viscoelastics, which, like a "third hand" for the surgeon, create volume inside the eye. Because of them, the eye does not flow out when several punctures are made in it.

Viscoelastic Viscoelastics are
visually transparent, they help to completely remove the entire lens, so that not the slightest fragment remains (left after destruction).
Although the booklets speak of a single puncture, there are actually at least two or three of them: auxiliary ones are needed for the surgeon to work with the second hand with tools such as a poker or a spatula. The poker is called "chopper" - it helps to break down dense fragments of the lens vertically and horizontally in order to reduce the ultrasonic load on the tissues and the mechanical load on the ligaments of the lens. The solutions and the resulting emulsion are washed out through a hollow ultrasonic needle and aspiration tubes. In general, the surgeon works on the knife and fork principle.
Also, to expand the flaccid pupil and tension the flaccid capsular ligaments, various hooks or rings can be placed through the micro-holes (and sometimes even sutures are applied to the structures of the eye and individual parts of the lens) - there are a great many such devices and they are needed in difficult, advanced cases. We didn't need all of this, but it's easy to become a candidate - if you make an appointment too late.
Next is the stage of removing the lens. To get to its insides (nucleus and cortex), the surgeon models a round hole in the lens in the form of a circle manually or with a special laser. This procedure is called circular capsulorhexis.
Formation of a continuous circular capsulorhexis (window in the lens)

Imagine, the surgeon makes an even circle with a hand, 6-7 mm in diameter, opening a capsule 30 microns thick (thinner than a human hair).
Completion of the formation of a continuous circular capsulorhexis

:

:
The shape, size and completion of the capsulorhexis is a very important part of the operation. If the surgeon is inept, then it is possible to break the capsule in no time, and this will make the operation complicated, and in some cases it is even impossible to finish it with phacoemulsification.
After the completion of the capsulorhexis, hydrodissection is carried out (the introduction of a small amount of a special liquid into the capsule of the lens of the eye to facilitate dissection) of the lens and its hydrodissection from the capsule bag.
The next stages are: hydropreparation (separation of the lens capsule from its bulk by the flow of fluid) and delineation (a jet of liquid is introduced into the layers of the lens and secretes the nucleus and cortex). At this time, the patient has a fog in front of the eye and the clarity deteriorates, only the sensation of light remains.
Hydrodissection and hydrodelineation

Phacoemulsification

Despite its solid (cartilaginous) consistency, it is impossible to simply take and pull out the lens - first you need to "grind" it. This is done with a special machine - a phacoemulsifier. Due to ultrasound, it fragments the lens to the state of "puree" and "sucks" it - like a vacuum cleaner with a slotted nozzle. If the lens is overripe and black in color, then the sounds when removed will be like a dentist's drill. If immature, initial - everything goes quickly, the device absorbs particles easily and ultrasound is used a minimum amount, and the surrounding tissues (cornea, iris, vitreous) remain healthy.
Phacoemulsification - a fragment of the lens on a needle

Aspiration, that is, the collection of biological material or fluid using an aspirator

, —

, —
After the work done, an empty space remains in the eye - a lens capsule, a kind of "pocket" in which an intraocular lens will soon be found. If we imagine the lens in the form of a grape, then the inner contents are removed and a transparent shell with a hole in the front wall remains.
Pay attention to two photographs: they differ in that in the first the pupil is red, and in the second it is black. In the first case, red light is still present on the lens - in fact, this is a reflex from the fundus with blood vessels. In the second case, the lens is no longer there and the tilt of the coaxial illuminator is different - without the lens the refraction changes and we no longer see the bottom - only the "hole" in the eye itself. Darkness, abyss)
Light versus darkness

Clean pocket ready for IOL implantation

In tweezers - the first lens, which is rolled up into a tube and placed in a disposable injector:

IOL loading and injection

Next, an injector is inserted into the previously made main puncture, which introduces the lens into the vacated space. Under the forces of its own elasticity (and possessing shape memory), the lens unfolds, and its "paws" rest against the edges of the lens capsule. The more legs, the better. The less space left in the bag, the better.
Further, the task of the surgeon is to correctly orient the lens along the axis of rotation. After some time, the lens will finally “sit down”, and the shape of the lens capsule will securely “embrace” it. Then the viscoprotector is washed out from under the lens (and above it) and it is ready.
Washing out viscoelastic after implantation

Everything. The same is done with the second eye.
About the lenses
The lens packaging lists its optical characteristics, as well as "instructions" for installation. The fact is that the lens installed in our case must compensate for such an optical defect of the eye as astigmatism - the "curvature" of the cornea, which previously had to be compensated for with glasses. That is, during the operation, they did not just put an artificial lens, but selected one that is better than the natural one in a number of parameters.
There are patients without astigmatism or when it is very small (up to ¾ diopters), then they have symmetrical lenses that can be twisted almost as desired. But if astigmatism is present (as a rule, it is from birth), then the lenses are made asymmetrical and they must be installed strictly at a certain angle relative to the eyes. For this, marks on the lens and time marks on the eye (which were applied with a marker) are used.

Crib complete with lens:
Nasal - side to nose (Latin os nasale)
Temporal - side of the temporal bone (Latin os temporale).
85 and 104 ° - just the angles of the astigmatic defect
Immediately after surgery
I was sitting in the waiting room with a laptop, working. Suddenly the door opens and either Kano from Mortal Kombat appears, or Jack Sparrow (CAPTAIN Jack Sparrow) without a hat - Dad came himself. One eye was sealed with a gauze bandage, the other was covered with a transparent plastic hemisphere to protect the eye from external mechanical influences. For post-operative eye care, a few drops and a special gel were prescribed.

Realizing that it was possible to go, we got behind the wheel and drove off - all the way Dad shared his impressions of the operation, comparing it according to various criteria with keratotomy. In short, progress in everything - in the time of the operation, in the amount of "damage", in the side effects, as a result of its predictability, in the time of rehabilitation - medicine has stepped right over several decades.
As in my case, a few days after the operation there were special effects - a slight haze, blurred images, halos around light sources. Most of it was gone within a week. A month later, there was only one small side effect, which is described as similar to chromatic aberration at the edges of some objects. Here is what Tatyana Yuryevna replied to this:
“These are optical effects that at first can be on multifocal lenses. But even monofocal lenses sometimes give such effects, neuroadaptation is needed. Moreover, after keratotomy, the cornea has notches that forever changed its shape. The edge of the IOL can give aberrations, the posterior capsule can give such dispersion, plus the epithelium, etc. The brain adapts and extinguishes the unnecessary image) ”
Then there were several planned examinations - they studied the process of eye restoration, measured its“ vision ”and adjusted the schedule for taking various drops. Everything is in order, vision is fully restored.

The full recovery time is 3 months - they have not yet passed, but all anomalies have practically disappeared.
Cube in a cube
Many of you know "Cube in a Cube" who have not watched the series with their voice acting. Do you know about a cube in a cube in a cube? ) It was such a gift as a token of gratitude that my father, a turner of the sixth grade, gave Tatyana) Something like a simplified eye model: the inner cube is the lens, the middle cube is the cornea, the large one is the eye itself.

If it was in Cuba, it would be a cube in a cube in a cube in Cuba.
To some, this product will seem complicated and he will look for welds or other dirty tricks. But a techie will easily understand in what sequence and how to do this on a lathe from a single piece of metal. What can not be said about the eye - everything is much more complicated there and it is better for a person not to meddle there once again.
The end
Two years have passed since I underwent surgery, but I still remember that feeling and emotions when I began to see the world in all its glory. And I am pleased that now my father is experiencing these feelings. And as a separate point, it's nice that nothing will happen to the new "lenses".
I don't want to philosophize and write something in the reviews - write better questions in the comments, we will try to answer everything. Well, for those who have finished reading, two pleasant bonuses:
- The code word " Habr " will give a small discount for primary diagnostics
- The code word " Bumburum " will give a 5% discount on the operation at Tatiana Shilova
Thank you all for your attention. Protect your eyesight and health!